> the previously approved transuranic radionuclide decontamination drug, diethylenetriamine pentaacetate (DTPA), can only be administered intravenously or by nebulizer—both of which are less feasible options for rapidly treating large populations than the oral route of HOPO 14-1.
Man, the hypothetical scenarios they used to get funding for this must have been horrific.
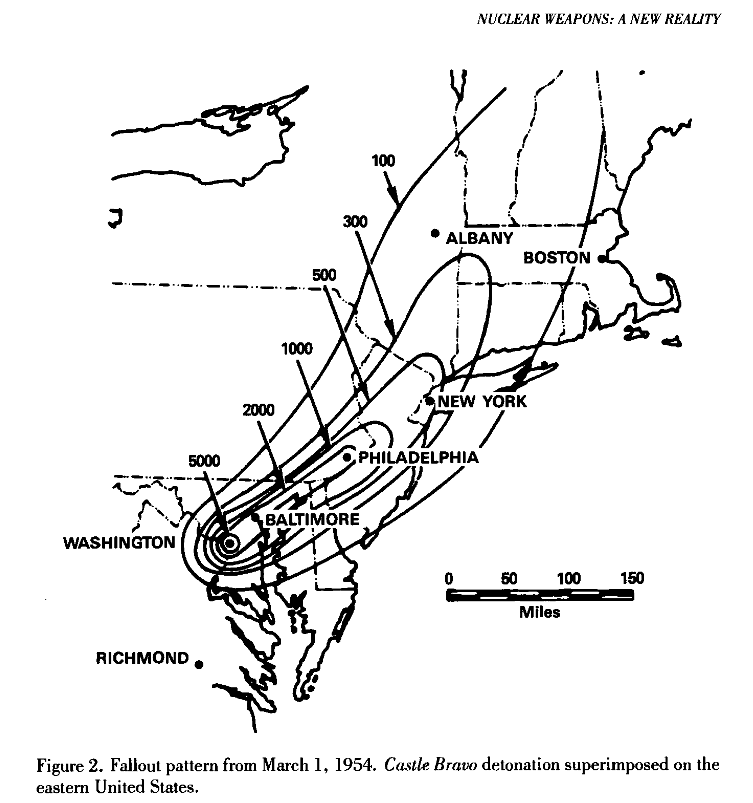
It's pretty striking that when they set off the Castle Bravo thermonuclear weapons test in the Pacific Ocean, someone superimposed the fallout map on the continental USA. If it had been dropped on DC, half of the population in NYC would have received a fatal dose from the fallout (if unsheltered).
Kinda nuts.
> "If Bravo had been detonated in Washington, D.C., instead of Bikini, Fields illustrated with a diagram, that lifetime dose in the Washington-Baltimore area would have been 5,000 roentgens; in Philadelphia, more than 1,000 roentgens; in New York City, more than 500, or enough to result in death for half the population if fully exposed to all the radiation delivered. This diagram was classified secret and received very little distribution beyond the Commissioners"
Yes but why would you? Radioactivity means you can't reoccupy the land yourself.
If dispensing misery is the goal, we have more effective chemical and biological weapons which are less militarily useful for the same reasons as a high-fallout nuclear bomb would be.
In a mutually assured destruction scenario, I don't think you could plausibly expect to invade the other country. The world as we know it would be over but some people would survive the exchange, maybe those in power could have a lot of spite and want to completely salt the earth with some cesium nukes to prevent the other country from recovering even after the nuclear winter subsides.
Why would they build the weapon in the first place though? MAD is a deterrence strategy: the weapon isn't meant to be used, but to work you must have sufficient weapons to ensure you get reliable kills on all your military targets.
If this is the plan, then building more weapons than that is a pointless waste of money because you're not planning to use them. If MAD isn't the plan, but rather hostage taking (ala North Korea) then a high fallout device is still useless because you have Assured Destruction if you launch it, but also not enough capability to ensure it arrives (the US can plausibly defend against a "rogue launch").
So again, when would you bother building it? At any given junction you either have enough weapons, or you need more warheads putting heat and overpressure on targets to ensure reliable kills and this deterrence.
Building a bunch of weapons which will cause at most tens of thousands of deaths months later, after you incinerate millions makes absolutely no economic sense and hence why at the height of the Cold War everyone looked at the concept and concluded it wasn't worth pursuing outside of a research analysis.
In a non-MAD employment scenario, you would build them for area denial. e.g. I don't really know how far the fallout would go from some cesium nukes, but maybe if russia wants a moat that lasts a long time but they can't take over ukraine with conventional forces, then they could launch some at ukraine and build their moat that way.
In a MAD scenario, I would view them as a bigger scarier stick to threaten people with.
And if it is ever needed, let's hope the stockpiles and logistics are in place to allow for quick distribution of the drug to broad portions of populations which are affected. We saw with COVID-19 that the U.S. let the Strategic National Stockpile become depleted. In the worst case, let's hope the drug has been maintained to be immediately available.
They're determining safety and tolerability, not efficacy. For this, they just need adequately compensated trial volunteers who take one of several different doses of the medicine and track/report symptoms, have some doctor visits, and get a lot of blood drawn. Oh, and for this one, sample urine and feces. You can read the clinical trial doc: https://clinicaltrials.gov/ct2/show/NCT05628961
To get full approval they could combine this with animal efficacy studies like they did for the smallpox treatment tecoviromat, since you can’t give smallpox to trial participants either. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6663070/
It turned out to be really useful to have tecoviromat for the recent mpox outbreak
This is cool. This is for removing nucleotides from the body, rather than repairing damage done by radiation exposure (which probably can’t be done with drugs).
This is factually incorrect. This HOPO 14-1 chelates f-block elements, many of which are radioactive, without depleting other metal ions from the body which are essential for metabolism and other functions. Also, there are a large number of agents which can mitigate the damage done by radiation exposure when administered prophylactically
Nuclear winter leading to crop failure and famine is still a terrifying specter. Even if there was a magical pill that made people 100% radiation proof that could be easily manufactured and distributed without any logistical problems, there would still be UNFATHOMABLE death and misery, and I think there’d still be pretty good odds that we’d go extinct.
{kind=link}
Man, the hypothetical scenarios they used to get funding for this must have been horrific.
Let's hope this drug is never needed.